No surgery. No scar. Under local anaesthesia.
Dr Nicolas Villard, an internationally recognised expert with over 1,000 treatments performed, offers minimally invasive thyroid nodule treatments by radiofrequency or microwave ablation in Geneva and Lausanne.
Procedure under local anaesthesia, no scar, outpatient or short hospitalisation
Performed by an interventional radiologist under real-time ultrasound guidance
65–85% volume reduction, supported by numerous scientific studies
Treatment reimbursed by mandatory health insurance (LAMal) in Switzerland
Thyroid function maintained after treatment — no need for lifelong hormone replacement
Over 1,000 treatments performed by Dr Villard, co-author of the French national guidelines
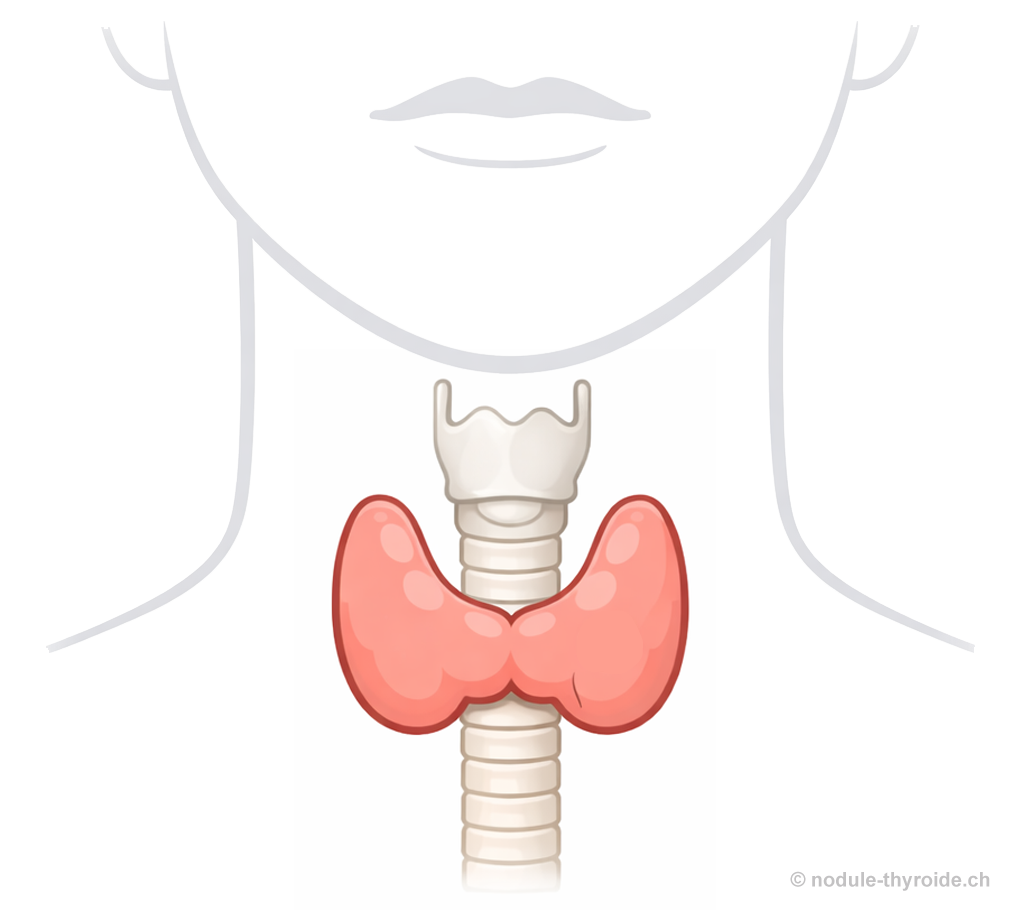
The thyroid is a small butterfly-shaped gland located at the base of the neck, in front of the trachea. It plays an essential role in the body's functioning by producing hormones (T3 and T4) that regulate metabolism — the rate at which the body uses energy.
These hormones influence body temperature, heart rate, weight, mood and concentration. A thyroid disorder can have a significant impact on health.
The parathyroid glands are small glands (usually four), located just behind the thyroid. They regulate blood calcium levels through a hormone called PTH (parathyroid hormone). Their proper functioning is essential for bones, muscles and the nervous system.
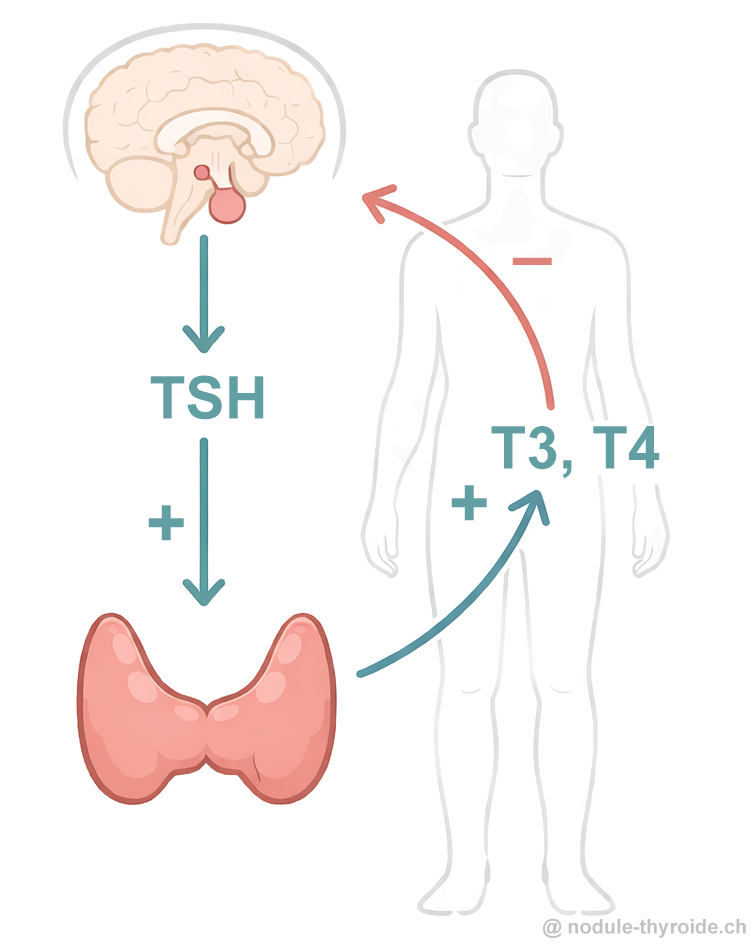
The thyroid does not function alone: it is regulated by a small gland in the brain called the pituitary gland, which controls the thyroid by producing TSH (Thyroid Stimulating Hormone).
When the body needs more thyroid hormones, the pituitary increases TSH production, stimulating the thyroid. Conversely, if thyroid hormone levels are too high, TSH production decreases. This feedback mechanism maintains a stable hormonal balance.
Hyperthyroidism occurs when the thyroid produces too many hormones (T3 and T4). This accelerates metabolism and can cause symptoms such as weight loss, nervousness, palpitations, unusual fatigue or heat intolerance. In hyperthyroidism, TSH levels are typically very low with elevated T3 and/or T4 levels.
Hypothyroidism occurs when the thyroid does not produce enough hormones (T3 and T4). Metabolism slows down, causing symptoms such as weight gain, significant fatigue, cold sensitivity, dry skin, constipation or poor concentration. In hypothyroidism, TSH is often elevated with low T3 and T4 levels.
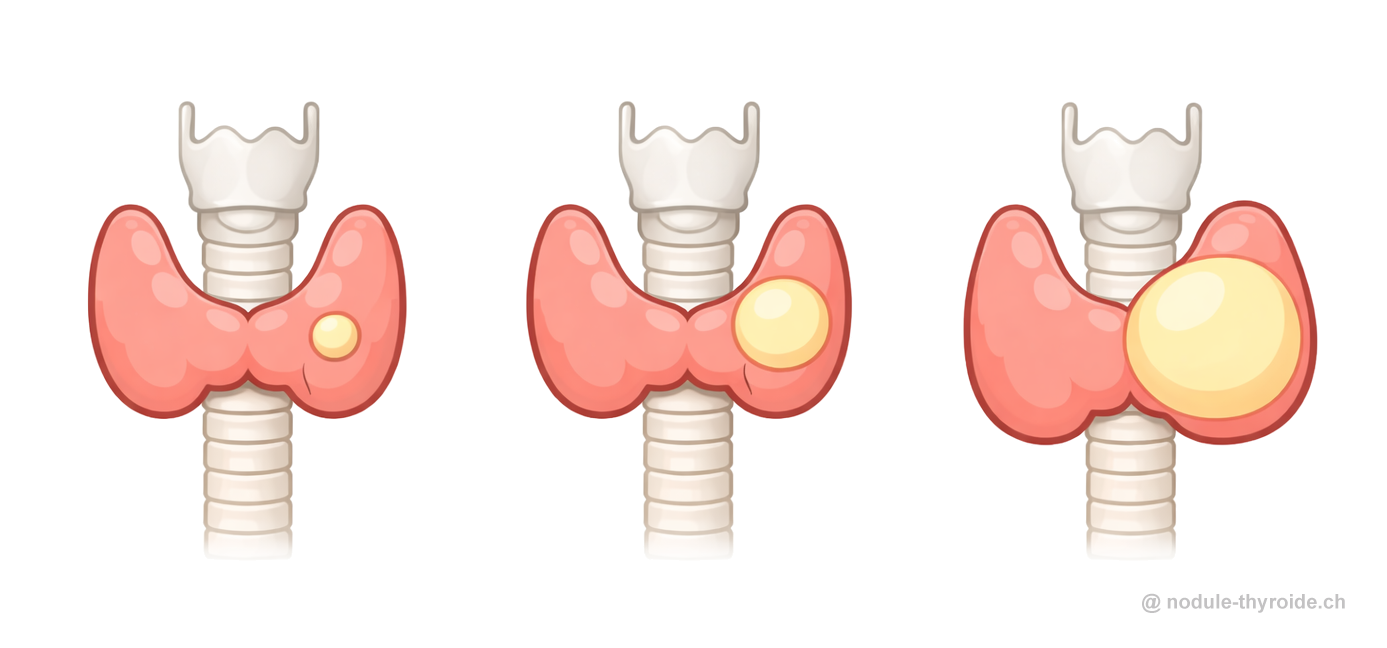
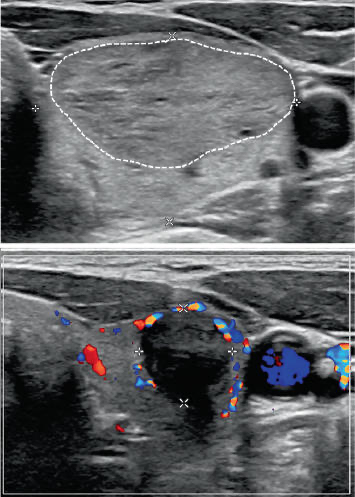
A thyroid nodule is a small lump that forms within the thyroid gland. This is a very common condition: approximately 30 to 50% of the population has at least one nodule detectable by ultrasound, but the vast majority (over 90%) are benign.
Nodules are often discovered incidentally, as they usually cause no symptoms. Some nodules may however cause symptoms related to their size (discomfort in the throat, difficulty swallowing) or excessive thyroid hormone production (toxic nodule).
Depending on their size and ultrasound appearance, some nodules will require a fine-needle aspiration (biopsy) to analyse their nature and exclude cancer. Initial evaluation is performed by an endocrinologist and/or radiologist.
This is the most common type. It does not produce thyroid hormones and is often discovered incidentally. It is called "cold" because it does not appear active on thyroid scintigraphy. Most do not require treatment if they remain stable in size and cause no symptoms.
When they are large or growing, they may cause cosmetic symptoms (neck swelling, visible mass) or compressive symptoms (discomfort, pressure in the neck, difficulty swallowing, dry cough).
In this case, the nodule produces thyroid hormones independently, without TSH control. It is called "hot" because it appears active on scintigraphy. It can cause hyperthyroidism with symptoms such as nervousness, weight loss or palpitations. This type of nodule is almost always benign.
Treatment is generally necessary because untreated hyperthyroidism can be dangerous, seriously affecting the heart, bones, brain and general health, particularly in elderly or frail patients.
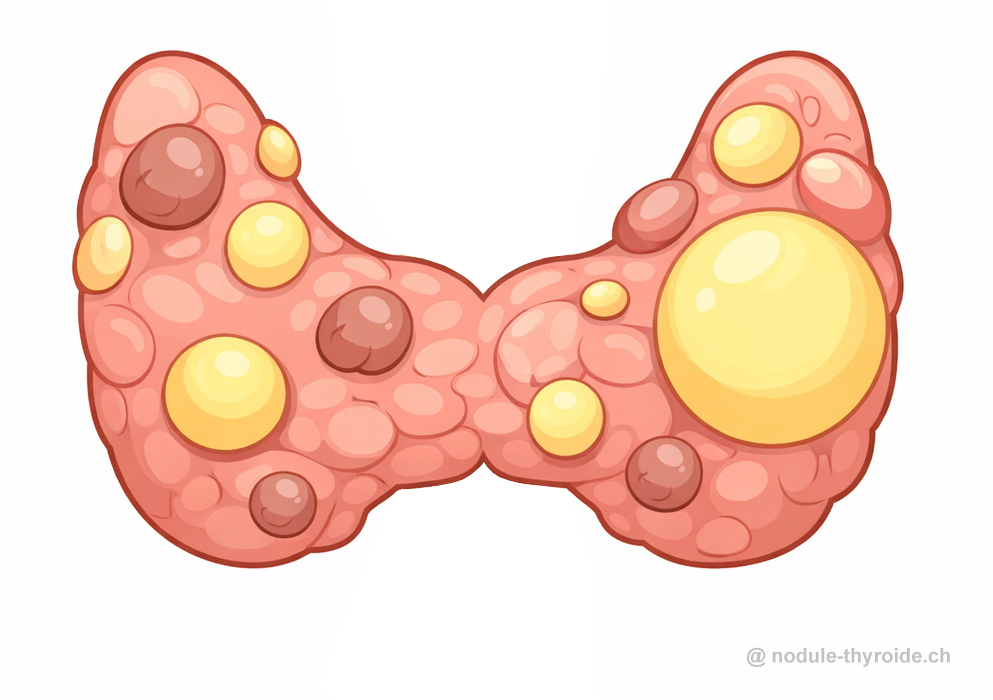
Multinodular goitre refers to an enlarged thyroid with multiple nodules. It is common, especially in elderly patients or those with a history of iodine deficiency. The goitre may be silent, cause compression, or lead to hyperthyroidism if it contains one or more autonomous nodules. Treatment depends on symptoms, volume and nodule function.
In a minority of cases (about 5–10%), a thyroid nodule may be cancerous. The most common type is papillary carcinoma, which generally has a good prognosis. Diagnosis is often suggested by ultrasound and confirmed by fine-needle aspiration.
The majority of thyroid cancers diagnosed today are low-risk forms — small, well-localised, and very slow-growing. In these cases, active surveillance (without immediate treatment) may be offered.
It is now possible to treat some of these small localised cancers with minimally invasive percutaneous techniques (radiofrequency, microwave or cryoablation), performed under image guidance by an interventional radiologist, without surgery or visible scarring.
This is not a thyroid nodule but a (virtually always) benign tumour of a parathyroid gland. It produces too much parathyroid hormone (PTH), causing hypercalcaemia. This can lead to fatigue, bone problems, kidney stones or digestive disorders. The standard treatment is surgical, but in an increasing number of cases, targeted minimally invasive radiofrequency treatment is feasible.
Minimally invasive treatments are most often performed under local anaesthesia. In some cases, particularly for children or very anxious patients, general anaesthesia may be used. A sterile environment (operating theatre or interventional radiology suite) is required.
When the target nodule is small and centrally located, treatment can be performed as an outpatient procedure. For larger nodules, particularly those that are subcapsular or near critical structures, a short hospitalisation is preferred for better post-operative monitoring.
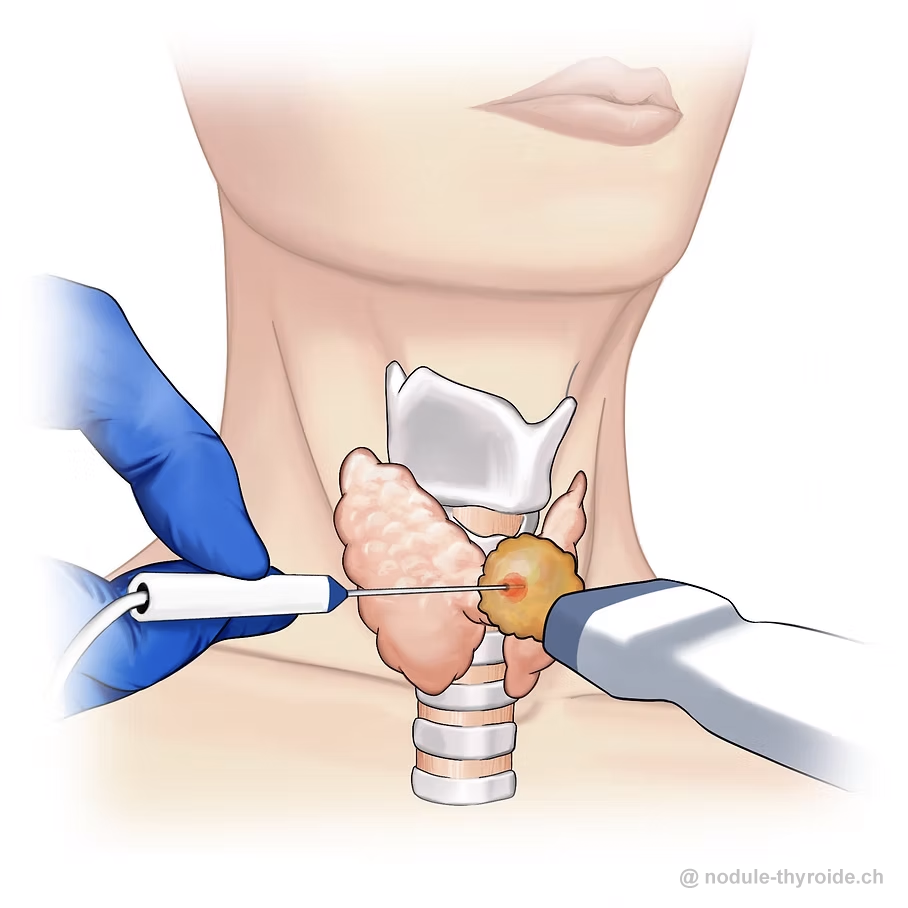
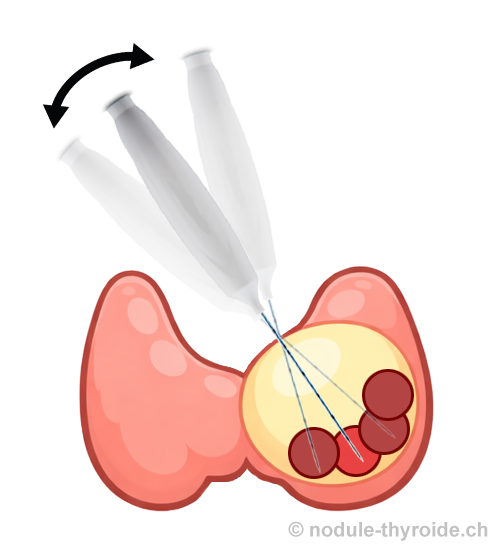
Thermoablation is a minimally invasive treatment that involves inserting a fine needle into the target lesion under imaging guidance (usually ultrasound). The needle tip generates heat to destroy the lesion. The operator performs multiple small ablations by moving the needle through the lesion for complete treatment. The cells are destroyed by heat, and the cellular debris is gradually resorbed by the body.
Two main technologies are used: radiofrequency ablation (RFA) and microwave ablation (MWA). Both techniques have comparable efficacy and safety. The only significant difference concerns contraindications: RFA is contraindicated during pregnancy, with cochlear implants, cardiac pacemakers or implanted defibrillators. In these situations, microwave ablation (MWA) is a safe alternative. Less commonly, cryoablation (a needle producing an ice ball) may be used when the lesion is adjacent to fragile structures that cannot be separated by hydrodissection.
Dr Villard has advanced the technique by systematically targeting complete nodule destruction, edge to edge. While most operators only destroy the central part of the nodule, this comprehensive approach combined with systematic hydrodissection makes regrowth virtually impossible.
Ethanol ablation is a minimally invasive method used mainly for thyroid nodules with a cystic (fluid) component. It involves aspirating the cyst fluid under ultrasound guidance and injecting a small amount of medical-grade ethanol. The alcohol destroys the inner wall of the cyst, preventing reaccumulation and causing gradual regression. Ethanol ablation may sometimes be combined with thermoablation.
Immediately after treatment, you will be monitored for a few hours. Occasionally, an overnight stay may be necessary.
Follow-up consultations with ultrasound are scheduled at 1 month, 3 months, 6 months, 12 months, 24 months, then long-term follow-up in collaboration with your referring endocrinologist. These appointments are essential to ensure complete treatment and detect any regrowth or recurrence.
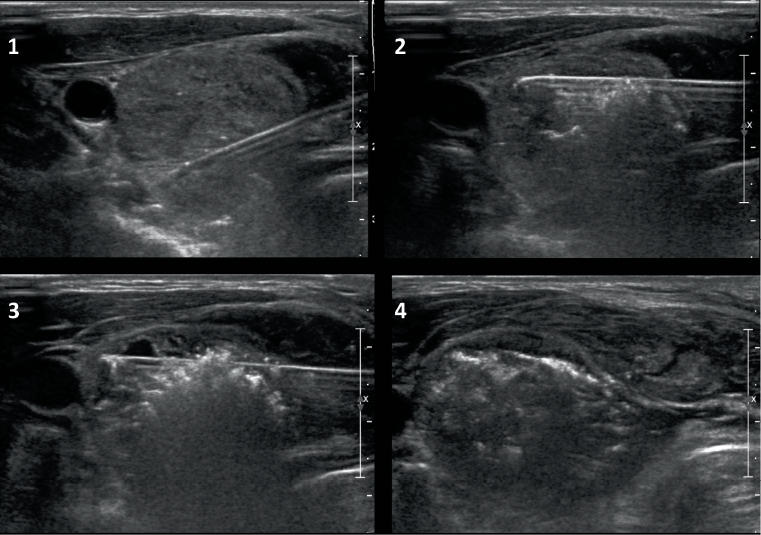
After treatment, the nodule gradually decreases in size. Significant reduction begins approximately 1 month after the procedure.
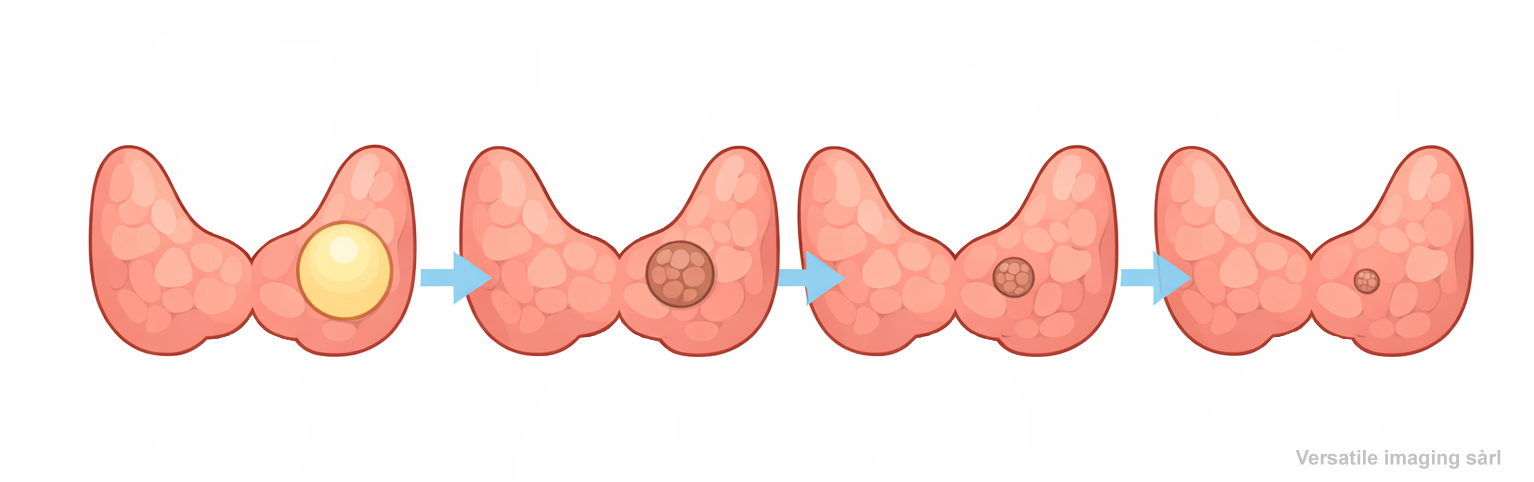
Progressive nodule evolution after thermoablation: 65–85% volume reduction
For autonomous ("hot") nodules, the hormonal issue is resolved immediately after treatment. Thyroid function is monitored during the first month.
It is important that the treating physician performs or supervises follow-up ultrasounds, as they can more easily assess nodule morphology and detect incomplete treatment or signs of recurrence.
Minimally invasive thyroid nodule treatments are generally very safe, with less than 1% of severe complications.
Minor bruising around the thyroid, mild neck discomfort or pain well managed with simple pain relief (Paracetamol or Ibuprofen). These typically resolve within a week. Return to work is usually possible after 1–2 days.
Transient recurrent laryngeal nerve involvement causing a hoarse or weakened voice. Recovery is progressive over weeks to months, often helped by speech therapy. Prognosis is always favourable.
Rare complication occurring days to weeks after the procedure. Presents as neck pain and local swelling. Outcome is generally favourable with conservative management.
Unlike surgery, normal thyroid tissue is spared. Hypothyroidism after minimally invasive treatment is exceptional.
| Criterion | Surgery | RFA |
|---|---|---|
| Hospitalisation | Yes (several days) | None or brief (outpatient possible) |
| Anaesthesia | General | Local |
| Scar | Yes | No |
| Risk of hypocalcaemia | Yes | No |
| Risk of voice changes | Higher | Lower |
| Risk of hypothyroidism | 100% (total thyroidectomy), 10–20% (lobectomy) | Very rare |
| Previous surgery | High complication risk | Easy repeat procedure |
| Lymph node metastases | Possible for nodes > 3 cm. Functional cervical dissection. | Limited to nodes < 3 cm visible on ultrasound |
| Inoperable patient | Not possible | Excellent candidate |

Interventional Radiologist specialising in thyroid
Dr Nicolas Villard is a Swiss physician specialised in interventional radiology with internationally recognised expertise in minimally invasive thyroid treatments.
He has performed over 1,000 treatments of thyroid nodules, making him the most experienced specialist in this field in Western Switzerland. He has refined the technique, notably with the systematic use of hydrodissection, ensuring optimal protection of structures adjacent to the thyroid.
He is co-author of the French guidelines for thyroid nodule treatment published by the French Society of Radiology (SFR), CERF and CIREOL.
He regularly presents at international conferences to share his expertise and organises training workshops for physicians several times a year.
He practises in several clinics in Lausanne and Geneva, in collaboration with endocrinologists throughout Switzerland. Consultations are available in French, English or German.
Clinique Générale Beaulieu
Chemin de Beau-Soleil 20, 1206 Geneva
Clinique Montchoisi · Chemin des Allinges 10, 1006 Lausanne
Clinique Amiia · Rue Centrale 19, 1003 Lausanne
Google Maps


For a consultation in Geneva or Lausanne, contact Dr Villard's office.
Please send your recent results (ultrasound, fine-needle aspiration, thyroid blood test (TSH, T3, T4)) to the office prior to your appointment.
Select a time slot online for a consultation in Geneva or Lausanne.